
Downloads
 Download
Download






This work is licensed under a Creative Commons Attribution 4.0 International License.
Review
Quantitative Risk Stratification Models for Coronary Heart Disease in Primary and Secondary Prevention
Jia Wei #, Qiang Yang #, lin Lin, Canzhan Zhu, and Jin Wei *
Department of Cardiology, The Second Affiliated Hospital, School of Medicine, Xi'an Jiaotong University, Xi'an, Shaanxi, China.
* Correspondence: weijin@mail.xjtu.edu.cn;Tel: +86 13572140118
# Jia Wei and Qiang Yang are equally contributed to the manuscript.
Received: 30 April 2023
Accepted: 13 June 2023
Published: 28 September 2023
Abstract: Coronary heart disease (CHD) is the most prevalent non-communicable disease globally and has high morbidity, mortality and healthcare cost. Thus early and precise risk stratification is an important issue in the detection, diagnosis and therapy for CHD. There are a number of primary screening tools and risk scores involving CHD risk factors for cardiovascular disease worldwide, such as Framingham Risk Score, World Health Organization/International Society of Hypertension and Cardiovascular disease (CVD) risk prediction charts (RiskWHO), American College of Cardiology/American Heart Association (ACC/AHA) pooled cohort equations (RiskACC/AHA), ADAPT Protocol for Cardiac Event Risk. Those models calculate CHD risk based on CHD risk factors, including age, gender, hypertension, and diabetes mellitus. This review will summarize the risk stratification models of CHD and related clinical evidence. It will also include a thorough analysis of the current risk stratification models and offer some advice for future risk stratification model development.
Keywords:
coronary heart disease risk scores primary and second prevention1. Introduction
Coronary heart disease (CHD) remains among the leading causes of death in global population. Countries all over the world are now bearing the huge economic and social burden of cardiovascular diseases [1,2]. The underlying pathology is atherosclerosis, which develops continuously over years. Acute coronary events (heart attack) usually occur suddenly and lead to death if there is no treatment. In the diagnosis of cardiovascular disease, the determination of cardiovascular risk is the basis for an effective intervention [1]. Therefore, early and precise estimation of the cardiovascular risk, based on risk equations, is very important. Risk scores are essential elements that enable precise diagnostic evaluation for guiding treatment, especially for clinicians with different background levels and across different district regions. In this review, we will focus on current risk assessment models for CHD primary and secondary prevention.
2. Risk Scores in Primary Prevention
2.1. Framingham Risk Score (RiskFRS)
The Framingham Risk Score is a gender-specific algorithm that estimates the 10-year cardiovascular risk of an individual. It was first developed from the Framingham Heart Study [3].The Framingham Risk Score has been validated in the United States; it has been validated in men and women, and in European Americans and African Americans [4]. Even though the calibration accuracy of the Framingham risk functions was not satisfactory, it was able to rank individuals from low-risk to high-risk, with the discrimination ability of at least 60% [5]. To increase the capability for predicting risk of stroke, transient ischemic attack (TIA) and heart failure, an updated model—Framingham General Cardiovascular Risk Score was released in 2008 [6]. For the U.S. population, the Framingham risk prediction algorithm appears to predict CHD risk reasonably well except for Native Americans [7].
The first Framingham Risk Score included age, sex, low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), blood pressure, diabetes, and smoking. It performed well and correctly predicted 10-year risk for CHD in American men and women of European and African descent. The updated version was modified to include dyslipidemia, age range, hypertension treatment, smoking, and total cholesterol (TC), and exclude diabetes. Ford et al. reported a large cohort of 11,611 patients from the NHANES III study. The result shows that 81.7%,15.5%, and 2.9% patients had a 10-year risk for CHD of <10%, 10–20% and higher than 20%, respectively. High risk was most commonly found in patients with advanced age, and was more common in men than in women [8]. For the French population, Framingham risk function predicted twice as many CHD events than in observed. The area under the Receiver Operator Characteristic (ROC) curve was 74%. The risk function has good discrimination between high risk and low risk subjects, but it is not valid for estimating absolute 10-year CHD risk [9]. Studies have shown that Framingham Risk Score is most useful for identifying people at high risk of ASCVD [10].
2.2. World Health Organization/International Society of Hypertension CVD Risk Prediction Charts (RiskWHO)
The World Health Organization (WHO) and the International Society of Hypertension (ISH) have formulated CVD risk prediction charts for use in different countries; it uses the best available mortality and risk factor data. The WHO/ISH risk profile estimates the 10-year risk of a fatal or non-fatal cardiovascular event based on sex, age, systolic blood pressure,TC, smoking status, and presence of diabetes [11]. It is the first model which enables the prediction of future heart attack risk for people living in low- and middle-income countries; it can be applied even in low resource settings [12]. Due to the paucity of data, risk prediction charts (RiskWHO) have been compiled not for individual countries but for 14 WHO epidemiological sub-regions. For each sub-region, two charts were developed, one set with cholesterol and the other set without cholesterol. The accuracy and predictive value of current risk prediction charts will be improved as more epidemiological data become available from individual countries.
The WHO/ISH model involved risk factors such as age, sex, smoking, blood pressure, blood cholesterol, and presence of diabetes as clinical entry points for cardiovascular risk prediction. A hypothetical cohort was created for each WHO subregion, consisting of people in each age and sex group. The age groups used were 30–44, 45–59, 60–69, and 70–79 years. Individuals were assigned values for the following cardiovascular risk factors: systolic blood pressure,TC, and smoking status. Estimates of relative risk per unit increase in continuous risk factors, i.e. per mmHg for systolic blood pressure and per mmol/L for TC, as well as for the presence of smoking were determined. These relative risk estimates were applied to the hypothetical cohort to determine the relative risk of each individual in the cohort. The probability of a cardiovascular event was extrapolated to a 10-year period. The mean absolute risk for various combinations of risk factor levels was then calculated and tabulated [13].
In 2015, Ghorpade et al. published a cross-sectional study including 570 subjects over 40 years old. Seventeen percent of the participants had moderate to high risk for the occurrence of cardiovascular events by using WHO/ISH risk prediction charts. CHD risk factors like smoking, alcohol, LDL-C, HDL-C were found in 32%, 53%, 56.3%, and 61.5% of study participants, respectively. This cross-sectional study indicates that WHO/ISH charts are easy and inexpensive tools for predicting cardiovascular events. The WHO/ISH risk prediction charts for the South-East Asian region were also validated [14].
2.3. American College of Cardiology/American Heart Association (ACC/AHA) Pooled Cohort Equations (Risk ACC/AHA)
In 2013 ACC/AHA guidelines, a new score was introduced to estimate the 10-year risk of developing a first ASCVD event. An ASCVD even was defined as nonfatal myocardial infarction (MI), CHD death, or fatal or nonfatal stroke. Follow up risk incorporates change in risk factor levels over time and requires both initial and follow up values. The information above helps with clinician-patient discussions on risk and risk-lowering interventions. For individuals with borderline or intermediate estimated 10-year risk, and patients reluctant to take medical therapy without clearer evidence of increased ASCVD risk, the assessment of ACC/AHA is a reasonable tool to reclassify risk either upward or downward as part of shared decision-making [15].
This score provides sex- and race-specific estimates for the first ASCVD event for black and white men and women aged 40-79 years. Variables that merit inclusion in the risk assessment equations are age, TC, HDL-C, systolic blood pressure (including treated or untreated status), diabetes, and current smoking status (Table 1).
Table 1. Risk ACC/AHA

In 2014, Than et al. [16] published a cohort of 4854 Rotterdam Study participants, the ACC/AHA model provided poor calibration and moderate to good discrimination. Improving risk predictions and setting appropriate population-wide thresholds are necessary to facilitate better clinical decision making.
2.4. China-PAR (Prediction for ASCVD Risk in China)
The China-PAR risk prediction model can be used to predict an individual's risk of developing ASCVD over a decade in Chinese patients, thereby aiding the prevention and management of cardiovascular disease [17]. ASCVD risk prediction equations were built by sex-specific Cox proportional hazards models, and the main risk factors included sex, age, current place of residence (urban or rural), geographical region (northern or southern, bounded by the Yangtze River), waist circumference, TC, HDL-C,blood pressure level, antihypertensive medication use, diabetes, smoking, and family history of CHD. Users can enter personal information into a website evaluation tool (http://www.cvdrisk.com.cn) or "cardio cerebrovascular risk" mobile app assessment tool and check the results. The China-PAR project developed and validated the first equations for 10-year ASCVD risk prediction in a Chinese population from large, contemporary, population-based Chinese cohorts. The sex-specific China-PAR equations had excellent performance of ASCVD risk prediction with good internal consistency and external validation accuracy [18].
This model adopted a 10-year risk division criteria as follows: low risk (<5%), medium risk (5%–9.9%) or high risk (≥10%). For lifetime risk, two groups are separated according to the following criteria: low risk (<32.8%) or high risk (≥32.8%) (Figure 1).
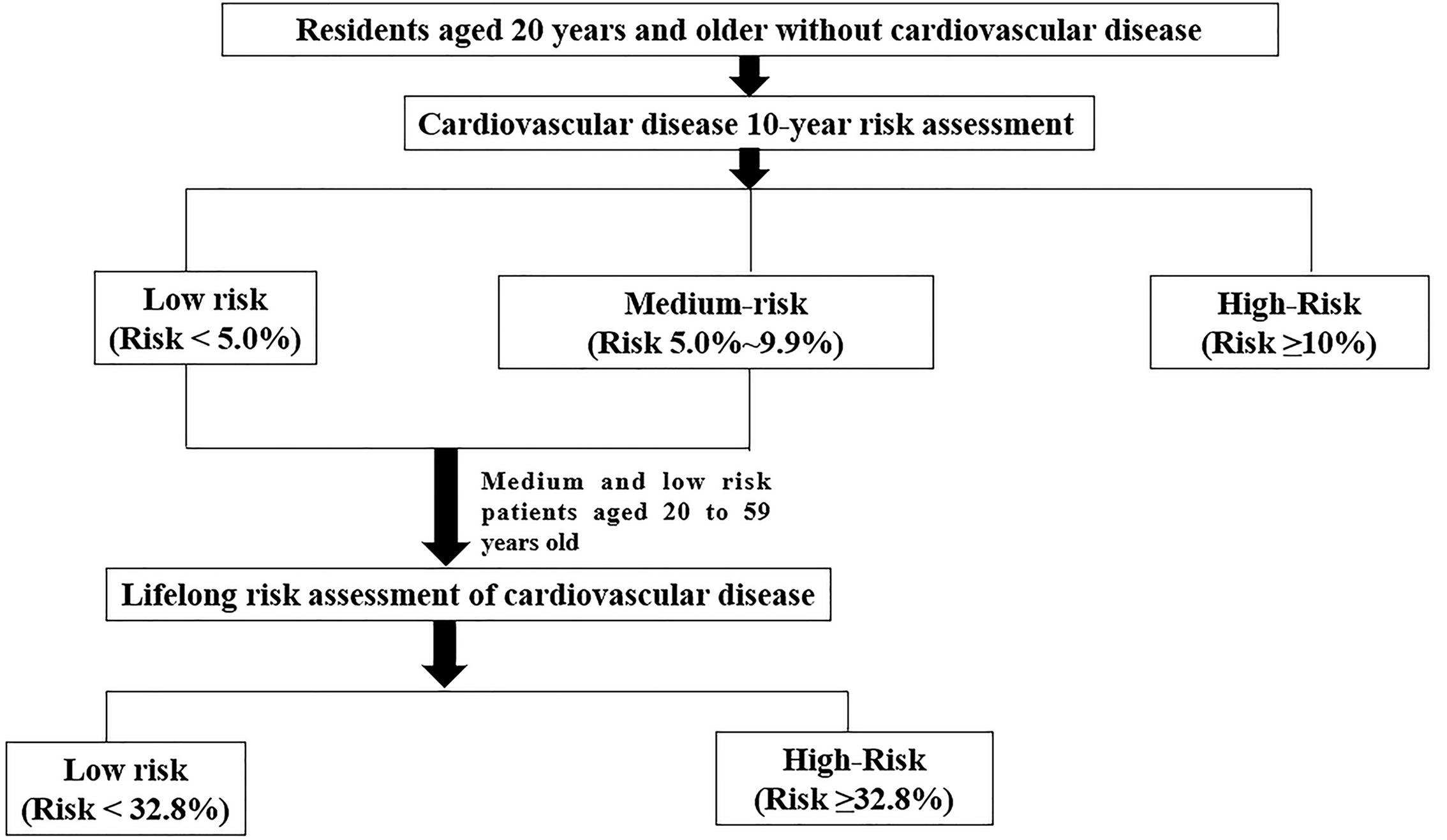
Figure 1. China-PAR model.
Yang et al. reported a validation cohort using the China-PAR equations. A total of 1922 ASCVD events were identified during an average follow-up of 14.1 years. The results show that ASCVD incidence increased more quickly among individuals with predicted 10-year ASCVD risk of >10%. After gender-specific analysis, there were no substantial differences between the observed and predicted incidence rates. The observed and predicted ASCVD event rates in men were 1.49% vs. 2.07%, 7.46% vs. 7.03%, and 16.52% vs. 16.23% across the three categories. Similar results were shown for women. This illustrated the good agreement between observation and prediction when participants were classified using predicted risk categories of <5%, 5–10%, and ≥10%. This method will be useful for self-management and prevention of ASCVD in Chinese adults [18].
2.5. QRISK Cardiovascular Disease Risk Score
To develop a new UK-appropriate cardiovascular risk score (QRISK) model, 1.28 million UK patients aged 35 to 74 years were enrolled in 318 clinics. The endpoints included MI,CHD, stroke, and transient ischemic attack. Risk factors were age, sex, smoking status, systolic blood pressure, TC/HDL-C ratio, body mass index, family history of CHD, socioeconomic deprivation and current antihypertensive drug therapy. The QRISK model is better suited to the UK population than the Framingham Risk Assessment or the previously published ASSIGN model.
Besides traditional risk factors such as age, sex, systolic blood pressure, smoking status, TC/HDL-C ratio that are included in the long-established Framingham equations, QRISK1 also includes body mass index, family history of cardiovascular disease, social deprivation (Townsend score), and use of antihypertensive treatment. Performance data indicated that QRISK1 is a more accurate tool to predict the development of cardiovascular disease in the United Kingdom compared with the Framingham equation [19]. QRISK2, the successor to QRISK1, is a new multivariable risk score that contains all the risk factors in QRISK1 and includes self-assigned ethnicity and conditions associated with cardiovascular risk (including diagnosed type 2 diabetes, treated hypertension, rheumatoid arthritis, renal disease, and atrial fibrillation) [20]. QRISK2 also contains interactions between age and Townsend score body mass index, systolic blood pressure, family history, smoking status, treated hypertension, diagnosis of type 2 diabetes, and atrial fibrillation. All continuous risk factors were carefully handled and kept continuous throughout the model building process, fractional polynomials were used to model nonlinear risk relations where appropriate.
A prospective open cohort study assessed the performance of the QRISK score and compared it with the Framingham score. QRISK performed better than Framingham in both discrimination and calibration capability. Framingham over-predicted 10-year CVD risk by 23% in the THIN cohort, while QRISK under-predicted the risk by 12%. The results suggest that QRISK is likely to provide more appropriate risk estimates than Framingham to help identify patients at high risk of CVD in the UK [21].
2.6. ASCVD Score
The ASCVD risk score is a national guideline developed by the American College of Cardiology. It calculates 10-year risk of having a cardiovascular problem, such as a heart attack or stroke. It takes three steps to calculate the ASCVD score. Step 1: High-Risk Criteria: History of ASCVD—History of acute coronary syndrome (ACS), MI, stable angina, coronary/other arterial revascularization, stroke, transient ischemic attack, or peripheral arterial disease (PAD) from atherosclerosis. Step 2: High-Risk Criteria: Extreme LDL—LDL-C≥4.92 mmol/L. Step 3: ASCVD Risk Criteria; Only Apply When LDL-C 1.81–4.90 mmol/L, including age, diabetic status, sex, race, TC, HDL-C, systolic blood pressure, treatment for hypertension, and smoking status.
Vidya et al. compared the ASCVD and FRS prediction value in a cohort with 1082 subjects, aged 18 to 39. FRS predicted 97% subjects as low (<10%) 10-year predicted risk and 4 participants as high predicted risk (>20%) of CVD. While ASCVD identified 61% with a high lifetime risk of developing CHD/stroke. The ASCVD score stratified 26.1% subjects into high 10-year risk while FRS classified 17.2% into high 10-year risk; the ASCVD risk estimator identified a larger proportion of subjects “at risk” of developing CVD. High prevalence of alcohol use, decreased intake of fruits and vegetables and low physical activity were observed in the “at risk” population. Using the ASCVD risk scoring tool we could better characterize the “at risk” subjects from the apparently asymptomatic cross-sectional population and personalize their risk (short term and long term) for developing CVD [22].
3. Risk Scores in Secondary Prevention
3.1. ADAPT Protocol for Cardiac Event Risk
The ADAPT Protocol for Cardiac Event Risk (ADAPT score) is used to assess the risk of cardiac events in patients experiencing two hours of chest pain. It helped to safely exclude MI and ACS within two hours of arrival at the emergency department (ED) in up to 20% of patients with chest pain. This significantly shortened the length of hospital stay without adverse consequences. It identified approximately half of the patients presenting to the ED with possible cardiac chest pain as having low risk of short-term major adverse cardiac events. This is a significant improvement compared to previously reported protocols [23].
The risk stratification model included abnormal troponin at 0 or 2 h, ischemic changes on electrocardiograph (ECG), age ≥65 years, ≥3 CHD risk factors (family history of CHD, hypertension, hypercholesterolemia, diabetes, or current smoker), known CHD (stenosis≥50%), aspirin use in past 7 days, severe angina (≥2 episodes in 24 h or persisting discomfort). Barring other concerning features for acute coronary syndrome or other life-threatening causes of chest pain (pneumothorax, pulmonary embolism, cardiac tamponade, aortic dissection, esophageal rupture, etc.), patients that meet the low-risk criteria can be considered for discharge with close follow-up after negative 0 h and 2 h troponin testing. Patients who do not meet the low-risk criteria should have MI excluded with serial ECGs and biomarkers.
A prospective observational study tested the ADAPT Protocol that included pre-test probability scoring by the Thrombolysis in Myocardial Infarction (TIMI) score, electrocardiography, and 0 + 2 h values of laboratory troponin I. In the 1975 patients with chest pain, the ADAPT protocol classified 392 patients as low risk and only one of them had major adverse cardiac events (MACE). Thus, the protocol had a sensitivity, negative predictive value, specificity and positive predictive value of 99.7%, 99.7%, 23.4% and 19.0%, respectively. This model is suitable for making rapid discharge decisions from the ED with early follow-up. This approach could also decrease the observation period required for some patients with chest pain [24].
3.2. HEART Score
The HEART score is an effective way to assess the risk of cardiovascular chest pain in the ED and ensure early treatment. It has helped emergency departments more easily identify patients who need intervention. It provides a holistic assessment of cardiogenic or non-cardiogenic chest pain in emergency patients, rather than limiting evidence to high-risk patients with acute coronary syndrome [25]. The limitation is that non-cardiogenic chest pain cannot be evaluated and diagnosed [26].
Patients with suspected ACS are evaluated with a standard ED focused history and evaluation based on five different variables, including history (H), 12-lead electrocardiogram (ECG; E), age (A), risk factors (R), and troponin (T)[27-29]. Each indicator of the HEART scoring system was assigned a score of 0, 1, and 2, respectively; the scores of the 5 indicators are added together to form the total score, which is between 0 and 10 points. A HEART score of 0-3 is defined as low risk, where the incidence of MACE is 0-2.5%, and discharge from hospital is permitted. A score of 4-6 was defined as moderate risk and the incidence of MACE was 12.0-16.6%; patients with this score required hospitalization for further examination. A score of ≥7 was defined as a high risk and the incidence of MACE was 50.0% to 65.0%, thus requiring emergency intervention [27, 30] (Table 2).
Table 2. HEART Score

Jain et al. found that the HEART score had relatively high short-term and long-term predictive value when evaluating low-risk patients with chest pain, with a near-term (within 30 days) MACE incidence of 0.6% and a long-term (within 5 years) MACE incidence of 10.0% [31]. Mahlar et al. found that the incidence of MACE decreased from 0.6% to 0 in patients with HEART score ≤3 in combination with 6 h sequential troponin test. The sensitivity and negative predicates of HEART score ≤3 were 99% and 98%, respectively, for predicting the incidence of MACE within 30 days. This means that the HEART score is highly predictive and evaluative of patients with chest pain [32]. Backus et al. prospectively verified TIMI, GRACE, and HEART scores in 2440 patients with chest pain. The results showed that the area under the ROC curve for HEART score was 0.83, which was significantly higher than the TIMI score of 0.75 and GRACE score of 0.70. Therefore, HEART score was the best scoring system for the evaluation of patients with chest pain in the emergency room [30].
3.3. GRACE Score
GRACE (Global Registry of Acute Coronary Events) risk scores can assess the risk and prognosis of ischemic adverse events in ACS patients and guide treatment strategies [33]. Parameters included age, systolic blood pressure, pulse, serum creatinine, Killip grade at presentation, cardiac arrest at admission, elevated markers of myocardial necrosis, and ST segment changes. If Killip grade or serum creatinine value is missing, renal failure and diuretic use can be added as scoring parameters. The cumulative score of each parameter is the GRACE score [34]. GRACE scores can stratify the risk of non-ST-segment elevation acute coronary syndromes (NSTE-ACS) patients and guide the selection of treatment strategies and the timing of interventional therapy. At the same time, ST segment elevation myocardial infarction (STEMI) patients can be classified into risk stratifications, with 0-109 as low risk, 109-140 as medium risk, and >140 as high risk. The higher the risk score, the greater the probability of a major adverse cardiovascular event within 1 year of discharge (Table 3).
Table 3. Treatment strategies were selected according to GRACE scores

Zhou et al. investigated the value of the GRACE score in predicting percutaneous coronary intervention (PCI) possibilities in NSTE-ACS patients. They recruited 80 consecutive patients, who presented with NSTE-ACS and received emergency coronary angiography (CAG) as well as emergency PCI. They found that PCI NSTE-ACS patients had significantly higher GRACE scores compared with NSTE-ACS patients without PCI. Then they used ROC curve to test whether the GRACE score is good at evaluating the possibilities of PCI in NSTE-ACS patients. The area under the curve was 0.854 ± 0.030 (P<0.001), indicating good predictive value. Furthermore, they analyzed results derived from ROC statistics, and found that a GRACE score of 125.5, as a cut-off, has high sensitivity and specificity in evaluating PCI possibilities in NSTE-ACS patients [35].
3.4. TIMI Score
TIMI (Thrombolysis In Myocardial Infarction) risk score is a scoring system used to assess the risk and prognosis of adverse events in patients with ACS. TIMI risk score included 7 measures [age ≥65 years, ≥ three CHD risk factors (hypertension, diabetes, family history of CHD, hyperlipidemia, smoking), known CHD (coronary stenosis ≥50%), aspirin use in the past 7 days, severe angina pectoris (≥2 episodes within 24 h), ST segment depression ≥0.5 mm and myocardial injury markers were increased]. Each item is 1 point and the highest possible total score is 7 points. Scores of 0-2 points is regarded as low risk, 3-4 points as medium risk, and 5-7 points is high risk. The higher the score, the higher the incidence of cardiovascular adverse events at 14 days [36].
For unstable angina (UA)/NSTE-ACS patients, the higher the TIMI score, the greater the probability of adverse events (for example, myocardial infarction, acute revascularization, and death). For STEMI patients, the higher the TIMI score, the greater the probability of a major adverse cardiovascular event within one year of discharge [34].
3.5. CRUSADE Bleeding Score
The CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress Adverse outcomes with Early implementation of the ACC/AHA guidelines) bleeding score is used to evaluate the likelihood of severe bleeding events occurring during hospitalization in ACS patients undergoing CAG. Patients can enter the link (https://m.medsci.cn/scale/show.do?id=e93e11059) for online assessment and calculate their CRUSADE bleeding score. The CRUSADE score is divided into five grades, from low to high risk: extremely low risk (<20 points), low risk (21-30 points), medium risk (31-40 points), high risk (41-50 points) and extremely high risk (>50 points). The corresponding bleeding risks are 3.1%, 5.5%, 8.6%, 11.9% and 19.5%, respectively. The higher the CRUSADE score, the higher the bleeding risk of patients, which can effectively predict the overall bleeding rate and is also effective in subgroup analysis [37].
4. Quantitative Risk Estimation in Current Prevention Guidelines and Drug Use
The 2018 AHA/ACC Cholesterol Clinical Practice Guidelines [38] recommend more detailed risk assessments for patients to help healthcare workers assess and make decisions about individualized risks and treatment options. Results of 10-year risk estimation should be communicated through a clinician-patient risk discussion to decide on the intensity of preventive measures, especially whether to initiate medical therapy. In present guidelines, patients with estimated 10-year ASCVD risk of 5% to <7.5% are considered to be at “borderline” risk and may be considered for drug therapy with a statin under certain circumstances; those with “intermediate” 10-year risk (7.5% to <20%) should be considered for initiation of moderate- to high-intensity statin therapy; and those with “high” 10-year risk (≥20%) should be considered for initiation of high-intensity statin therapy [38]. Some special groups, such as patients with familial hypercholesterolemia, should not be assessed using the existing risk score and often require intensive lipid-lowering medication.
Statin therapy is one of the most important preventive measures and has been recommended for patients who are at high risk for development of future CVD. Different guidelines recommend statin therapy for high risk subgroups as identified by using different risk score calculators. Studies have shown that the QRISK2 risk assessment model works well in the Indian population [10]. The HOPE-3 study [39] confirmed that rosuvastatin cholesterol-lowering therapy combined with antihypertensive therapy significantly reduced the risk of major cardiovascular events in people at moderate risk of ASCVD.
High-intensity statins reduce the risk of ASCVD by more than a third than moderate-intensity statins, so they are more beneficial for high-risk ASCVD patients. Therefore, for high-risk patients with ASCVD, whether secondary prevention or primary prevention, the 2018 AHA/ACC Cholesterol Clinical Practice Guidelines set the goal of reducing LDL-C by 50% or more, and use high-intensity statins when conditions permit. However, a few patients use high-intensity statins with many potential risks, including muscle-related adverse reactions, the development of diabetes, multiple drug reactions, treatment costs, etc. In the JUPITER study [40], the incidence of new diabetes was 3% in the rosuvastatin group and 2.4% in the placebo group (P=0.01). If high intensity statins are not tolerated, it is necessary to replace high intensity statins with low or medium intensity statins, and non-statin drugs can be added to reduce LDL-C levels. Available non-statin drugs include Ezetimibe, Bile acid chelator and Proprotein convertase subtilisin/Kexin type 9 (PCSK9) inhibitors [41].
5. Discussion
Risk assessment strategies are generally built based on economically viable parameters such as age, sex, blood pressure, blood lipids, blood glucose, smoking, and weight. Those traditional variables should remain the primary reference indicators for cardiovascular risk assessment in the near future. However, several issues must be noticed during development and implementation of CVD risk assessment. Firstly, cardiovascular disease spectrum and risk factors distribution differs significantly in different geographical regions, thus many reports found that specialized risk models, which are optimized based on regional population cohort are crucial for precise risk assessment [29, 30]. With the development of the economy, and medical diagnostic and therapy choices, both risk factors and disease prognosis are changing dramatically. Thus, the risk evaluation models need to be updated. Secondly, consensus is needed in endpoint choice during risk model development. Difference in endpoints posed great difficulty in model comparison and clinical use. For risk scores in primary prevention, 10-year ASCVD event risk is generally adopted as the endpoint. We suggest that the risk of cardiogenic events, cerebrovascular events and peripheral vascular events should be classified and calculated respectively if it was practicable. While in secondary prevention, it depends on the specific scenario for endpoint choice. In the emergency department, risk models for severe cardiovascular events have been developed. However, more models are needed to aid drug choice and intervention decision-making. Thirdly, more risk factors need to be included into risk stratification models during secondary prevention. New cardiovascular risk factors have been found and studied, such as carotid intima-media thickness, ankle-brachial index, homocysteine, coronary artery calcification and electrocardiogram exercise test.
In recent years, clinicians have many different evaluation options for patients with ASCVD, such as ultrasound, computed tomography, magnetic resonance imaging, electrocardiography and digital subtraction angiography. Quantitative plaque parameters by coronary CTA (CCTA) were associated with composite endpoints at multivariable analysis. Elevated non-calcified plaque volume, expressed as dichotomic variable, was associated with all combined endpoints [42]. CCTA offers the opportunity to visualize the coronary arteries in a complete fashion, including the arterial wall, vessel dimensions, tortuosity, and plaques with or without calcification. Specific plaque features such as positive remodeling, low-attenuation plaque, napkin-ring sign, and spotty calcification found in CCTA images have been identified as predictors of plaque rupture and acute coronary syndromes [43, 44]. CCTA can help to determine the characteristics of the plaque and predict coronary plaque rupture. Studies show that Napkin ring sign (NRS) in CCTA may help to characterize the risk prediction of coronary plaque rupture [45].
The PARADIGM registry study [46] reported that an average 10-year ASCVD risk was 11.3±9.9%. Plaque volume measured on baseline CCTA was significantly increased in the high-risk group compared with those in the moderate/low risk group. The development of total plaque/calcified plaque/non-calcified plaque was significantly correlated in the high-risk group compared with the moderate/low-risk group. Many of those evaluation tools provide abundant morphological and functional information. Compare those new risk factors and try to integrate them into the risk stratification model will help clinicians choose appropriate examination tools for different patients.
6. Conclusion
Cardiovascular disease is a serious disease that endangers people's health and life, with a high mortality rate and high disability rate. Although the pathogenesis of cardiovascular disease is still being studied, its main risk factors have been identified. Many studies have confirmed that hypertension, dyslipidemia (mainly increased cholesterol), diabetes, obesity, smoking, lack of physical activity and unhealthy eating habits are major and changeable risk factors for cardiovascular disease. With accumulating research on the mechanism of cardiovascular disease, more and more risk factors are included in the risk assessment model. At present, there are many quantitative risk stratification models to evaluate cardiovascular disease risk stratification, but there are also many deficiencies that need to be addressed. To further improve the accuracy of cardiovascular disease assessment, we need to further refine the population classification and develop individualized interventions and treatment plans for different individuals. In summary, there is still a long way to go in the development of cardiovascular disease risk assessment systems.
Author Contributions: Conceptualization, Jia Wei and Qiang Yang; validation, Lin Lin, Canzhan Zhu. and Jin Wei; writing—original draft preparation, Jia Wei.; writing—review and editing, Qiang Yang.; supervision, Canzhan Zhu.; project administration, Jin Wei; funding acquisition, Qiang Yang. All authors have read and agreed to the published version of the manuscript.
Funding: 2020 Natural Science Basic Research Program of Shaanxi Province, General Project (Youth)(ID:2020JQ-538)
Data Availability Statement: Not applicable.
Conflicts of Interest: The authors declared no conflicts of interests.

References
- Mihaylova, B. ;Emberson, J. ;Blackwell, L. ; et al . The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials . Lancet , 2012 , 380 ( 9841 ): 581 - 590 . doi: 10.1016/S0140-6736(12)60367-5
- Lloyd-Mostyn, R . National service framework for coronary heart disease . Ambiguities need to be clarified. BMJ. , 2000 , 321 ( 7261 ): 634 . doi: 10.1136/bmj.321.7261.634
- Wilson, P.W. ;D'Agostino, R.B. ;Levy, D. ; et al . Prediction of coronary heart disease using risk factor categories . Circ. J. , 1998 , 97 ( 18 ): 1837 - 1847 . doi: 10.1161/01.CIR.97.18.1837
- D'Agostino, R.S. ;Grundy, S. ;Sullivan, L.M. ; et al . Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation . JAMA. , 2001 , 286 ( 2 ): 180 - 187 .
- Reissigova, J. ;Tomeckova, M . State of the art coronary heart disease risk estimations based on the Framingham heart study . Cent. Eur. J. Public Health , 2005 , 13 ( 4 ): 180 - 186 .
- D'Agostino, R.S. ;Vasan, R.S. ;Pencina, M.J. ; et al . General cardiovascular risk profile for use in primary care: the Framingham Heart Study . Circ. J. , 2008 , 117 ( 6 ): 743 - 753 . doi: 10.1161/CIRCULATIONAHA.107.699579
- D'Agostino, R.S. ;Grundy, S. ;Sullivan, L.M. ; et al . Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation . JAMA , 2001 , 286 ( 2 ): 180 - 187 . doi: 10.1001/jama.286.2.180
- Ford, E.S. ;Giles, W.H. ;Mokdad, A . H . The distribution of 10-Year risk for coronary heart disease among U.S. adults : Findings from the National Health and Nutrition Examination Survey III. J. Am. Coll. Cardiol. , 2004 , 43 ( 10 ): 1791 - 1796 . doi: 10.1016/j.jacc.2003.11.061
- Vergnaud, A.C. ;Bertrais, S. ;Galan, P. ; et al . Ten-year risk prediction in French men using the Framingham coronary score: results from the national SU.VI.MAX cohort . Prev. Med. , 2008 , 47 ( 1 ): 61 - 65 . doi: 10.1016/j.ypmed.2008.02.023
- Garg, N. ;Muduli, S.K. ;Kapoor, A. ; et al . Comparison of different cardiovascular risk score calculators for cardiovascular risk prediction and guideline recommended statin uses . Indian Heart J. , 2017 , 69 ( 4 ): 458 - 463 . doi: 10.1016/j.ihj.2017.01.015
- Collins, D. ;Lee, J. ;Bobrovitz, N. ; et al . whoishRisk – an R package to calculate WHO/ISH cardiovascular risk scores for all epidemiological subregions of the world [version 2; peer review: 3 approved] . F1000Research. , 2017 , 5 : 2522 . doi: 10.12688/f1000research.9742.2
- Mendis, S. ;Lindholm, L.H. ;Mancia, G. ; et al . World Health Organization (WHO) and International Society of Hypertension (ISH) risk prediction charts: assessment of cardiovascular risk for prevention and control of cardiovascular disease in low and middle-income countries . J. Hypertens. , 2007 , 25 ( 8 ): 1578 - 1582 . doi: 10.1097/HJH.0b013e3282861fd3
- Selvarajah, S. ;Kaur, G. ;Haniff, J. ; et al . Comparison of the Framingham Risk Score, SCORE and WHO/ISH cardiovascular risk prediction models in an Asian population . Int. J. Card. , 2014 , 176 ( 1 ): 211 - 218 . doi: 10.1016/j.ijcard.2014.07.066
- Ghorpade, A.G. ;Shrivastava, S.R. ;Kar, S.S. ; et al . Estimation of the Cardiovascular Risk Using World Health Organization/International Society of Hypertension (WHO/ISH) Risk Prediction Charts in a Rural Population of South India . Int. J. Health. Policy. Manag. , 2015 , 4 ( 8 ): 531 - 536 . doi: 10.15171/ijhpm.2015.88
- Bittner, V . The New 2019 AHA/ACC Guideline on the Primary Prevention of Cardiovascular Disease . Circ. J. , 2020 , 142 ( 25 ): 2402 - 2404 . doi: 10.1161/CIRCULATIONAHA.119.040625
- Kavousi, M. ;Leening, M . J .G.; Nanchen D. ; et al. Comparison of Application of the ACC/AHA Guidelines, Adult Treatment Panel III Guidelines, and European Society of Cardiology Guidelines for Cardiovascular Disease Prevention in a European Cohort. JAMA, 2014 , 311 ( 14 ): 1416 - 1423 . doi: 10.1001/jama.2014.2632
- Yang, X. ;Li, J. ;Hu, D. ; et al . Predicting the 10-Year Risks of Atherosclerotic Cardiovascular Disease in Chinese Population: The China-PAR Project (Prediction for ASCVD Risk in China) . Circ. J. , 2016 , 134 ( 19 ): 1430 - 1440 . doi: 10.1161/CIRCULATIONAHA.116.022367
- Yang, X.L. ;Chen, J.C. ;Li, J.X. ; et al . Risk stratification of atherosclerotic cardiovascular disease in Chinese adults . Chronic. Dis. Transl. Med. , 2016 , 2 ( 2 ): 102 - 109 . doi: 10.1016/j.cdtm.2016.10.001
- Collins, G S ,Altman, D G . An independent and external validation of QRISK2 cardiovascular disease risk score: a prospective open cohort study . BMJ. , 2010 , 340 : c2442 . doi: 10.1136/bmj.c2442
- Hippisley-Cox, J. ;Coupland, C. ;Vinogradova, Y. ; et al . Predicting cardiovascular risk in England and Wales: prospective derivation and validation of QRISK2 . BMJ , 2008 , 336 ( 7659 ): 1475 - 1482 . doi: 10.1136/bmj.39609.449676.25
- Hippisley-Cox, J. ;Coupland, C. ;Vinogradova, Y. ; et al . Performance of the QRISK cardiovascular risk prediction algorithm in an independent UK sample of patients from general practice: a validation study . Heart , 2008 , 94 ( 1 ): 34 - 39 . doi: 10.1136/hrt.2007.134890
- Menon, V.P. ;Edathadathil, F. ;Sathyapalan, D. ; et al . Assessment of 2013 AHA/ACC ASCVD risk scores with behavioral characteristics of an urban cohort in India: Preliminary analysis of Noncommunicable disease Initiatives and Research at AMrita (NIRAM) study . Medicine , 2016 , 95 ( 49 ). doi: 10.1097/MD.0000000000005542
- Than, M. ;Flaws, D. ;Sanders, S. ; et al . Development and validation of the Emergency Department Assessment of Chest pain Score and 2 h accelerated diagnostic protocol . Emerg. Med. Australas. , 2014 , 26 ( 1 ): 34 - 44 .
- Than, M. ;Cullen, L. ;Aldous, S. ; et al . 2-Hour accelerated diagnostic protocol to assess patients with chest pain symptoms using contemporary troponins as the only biomarker: the ADAPT trial . J. Am. Coll. Cardiol. , 2012 , 59 ( 23 ): 2091 - 2098 . doi: 10.1016/j.jacc.2012.02.035
- Amsterdam, E.A. ;Wenger, N.K. ;Brindis, R.G. ; et al . 2014 AHA/ACC Guideline for the Management of Patients With Non–ST-Elevation Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines . J. Am. Coll. Cardiol. , 2014 , 64 ( 24 ): e139 - e228 .
- Long, B. ;Oliver, J. ;Streitz, M. ; et al . An end-user's guide to the HEART score and pathway . Am. J. Emerg. Med. , 2017 , 35 ( 9 ): 1350 - 1355 . doi: 10.1016/j.ajem.2017.03.047
- Six, A.J. ;Cullen, L. ;Backus, B.E. ; et al . The HEART score for the assessment of patients with chest pain in the emergency department: a multinational validation study . Crit. Pathw. Cardiol. , 2013 , 12 ( 3 ): 121 - 126 . doi: 10.1097/HPC.0b013e31828b327e
- Backus, B.E. ;Six, A.J. ;Kelder, J.C. ; et al . Chest pain in the emergency room: a multicenter validation of the HEART Score . Crit. Pathw. Cardiol. , 2010 , 9 ( 3 ): 164 - 169 . doi: 10.1097/HPC.0b013e3181ec36d8
- Six, A.J. ;Backus, B.E. ;Kelder, J . C . Chest pain in the emergency room: value of the HEART score. Neth. Heart. J. , 2008 , 16 ( 6 ): 191 - 196 . doi: 10.1007/BF03086144
- Backus, B.E. ;Six, A.J. ;Kelder, J.C. ; et al . A prospective validation of the HEART score for chest pain patients at the emergency department . Int. J. Card. , 2013 , 168 ( 3 ): 2153 - 2158 . doi: 10.1016/j.ijcard.2013.01.255
- Jain, T. ;Nowak, R. ;Hudson, M. ; et al . Short- and Long-Term Prognostic Utility of the HEART Score in Patients Evaluated in the Emergency Department for Possible Acute Coronary Syndrome . Crit. Pathw. Cardiol. , 2016 , 15 ( 2 ). doi: 10.1097/HPC.0000000000000070
- Mahler, S.A. ;Hiestand, B.C. ;Goff, D.C. ; et al . Can the HEART Score Safely Reduce Stress Testing and Cardiac Imaging in Patients at Low Risk for Major Adverse Cardiac Events? . Crit. Pathw. Cardiol. , 2011 , 10 ( 3 ). doi: 10.1097/HPC.0b013e3182315a85
- Members, A . T . F .; Hamm C.W.; Bassand J.;et al. ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation : The Task Force for the management of acute coronary syndromes (ACS) in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart. J. , 2011 , 32 ( 23 ): 2999 - 3054 .
- Roffi, M. ;Patrono, C. ;Collet, J. ; et al . 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC) . Eur. Heart. J. , 2016 , 37 ( 3 ): 267 - 315 . doi: 10.1093/eurheartj/ehv320
- Zhou, B.D. ;Zu, L.Y. ;Mi, L. ; et al . An analysis of patients receiving emergency CAG without PCI and the value of GRACE score in predicting PCI possibilities in NSTE-ACS patients . J. Geriatr. Cardiol. , 2015 , 12 ( 3 ): 246 - 250 .
- Antman, E.M. ;Cohen, M. ;Bernink, P . J .L.M.; et al. The TIMI Risk Score for Unstable Angina/Non–ST Elevation MIA Method for Prognostication and Therapeutic Decision Making. JAMA , 2000 , 284 ( 7 ): 835 - 842 . doi: 10.1001/jama.284.7.835
- Abu-Assi, E. ;Gracía-Acuña, J.M. ;Ferreira-González, I. ; et al . Evaluating the Performance of the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines (CRUSADE) Bleeding Score in a Contemporary Spanish Cohort of Patients With Non–ST-Segment Elevation Acute Myocardial Infarction . Circ. J. , 2010 , 121 ( 22 ): 2419 - 2426 . doi: 10.1161/CIRCULATIONAHA.109.925594
- Grundy, S.M. ;Stone, N.J. ;Bailey, A.L. ; et al . 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines . Circ. J. , 2019 , 139 ( 25 ): e1082 - e1143 . doi: 10.1161/CIR.0000000000000698
- Yusuf, S. ;Bosch, J. ;Dagenais, G. ; et al . Cholesterol Lowering in Intermediate-Risk Persons without Cardiovascular Disease . N. Engl. J. Med. , 2016 , 374 ( 21 ): 2021 - 2031 .
- Ridker, PM. ;Danielson, E. ;Fonseca, FA. ; et al . Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein . N. Engl. J. Med. , 2008 , 359 ( 21 ): 2195 - 207 . doi: 10.1056/NEJMoa0807646
- Grundy, SM. ;Stone, NJ. ;Blumenthal, RS. ; et al . High-Intensity Statins Benefit High-Risk Patients: Why and How to Do Better . Mayo. Clin. Proc. , 2021 , 96 ( 10 ): 2660 - 2670 . doi: 10.1016/j.mayocp.2021.02.032
- Andreini, D. ;Magnoni, M. ;Conte, E ; et al . Coronary Plaque Features on CTA Can Identify Patients at Increased Risk of Cardiovascular Events . JACC Cardiovasc Imaging , 2020 , 13 ( 8 ): 1704 - 1717 . doi: 10.1016/j.jcmg.2019.06.019
- Chang, H.J. ;Lin, F.Y. ;Lee, S.E. ; et al . Coronary Atherosclerotic Precursors of Acute Coronary Syndromes . J. Am. Coll. Cardiol. , 2018 , 71 ( 22 ): 2511 - 2522 .
- Motoyama, S. ;Sarai, M. ;Harigaya, H. ; et al . Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome . J. Am. Coll. Cardiol. , 2009 , 54 ( 1 ): 49 - 57 . doi: 10.1016/j.jacc.2009.02.068
- Maurovich-Horvat, P. ;Ferencik, M. ;Voros, S. ; et al . Comprehensive plaque assessment by coronary CT angiography . Nat. Rev. Cardiol. , 2014 , 11 ( 7 ): 390 - 402 . doi: 10.1038/nrcardio.2014.60
- Han, D. ;Berman, D.S. ;Miller, R . J .H.; et al. Association of Cardiovascular Disease Risk Factor Burden With Progression of Coronary Atherosclerosis Assessed by Serial Coronary Computed Tomographic Angiography. JAMA Netw. Open , 2020 , 3 ( 7 ): e2011444 . doi: 10.1001/jamanetworkopen.2020.11444


